.png)
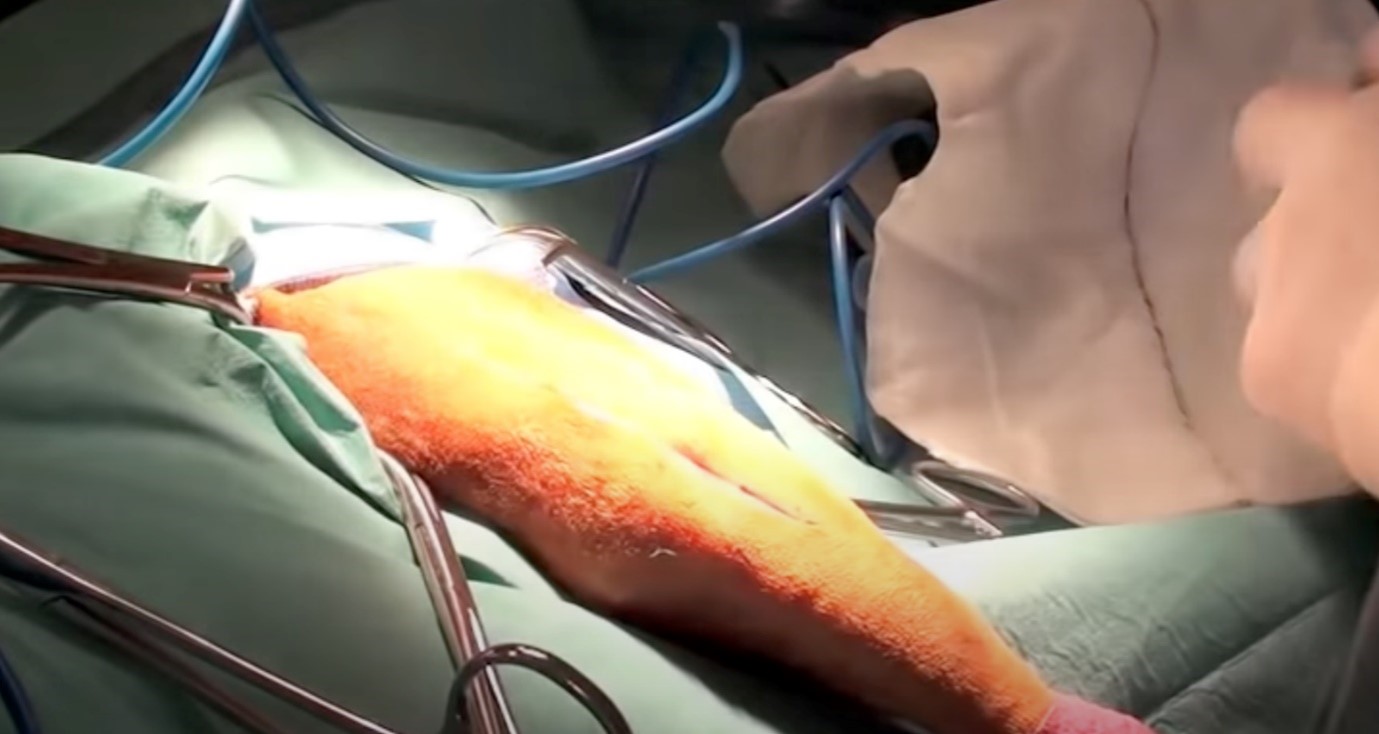
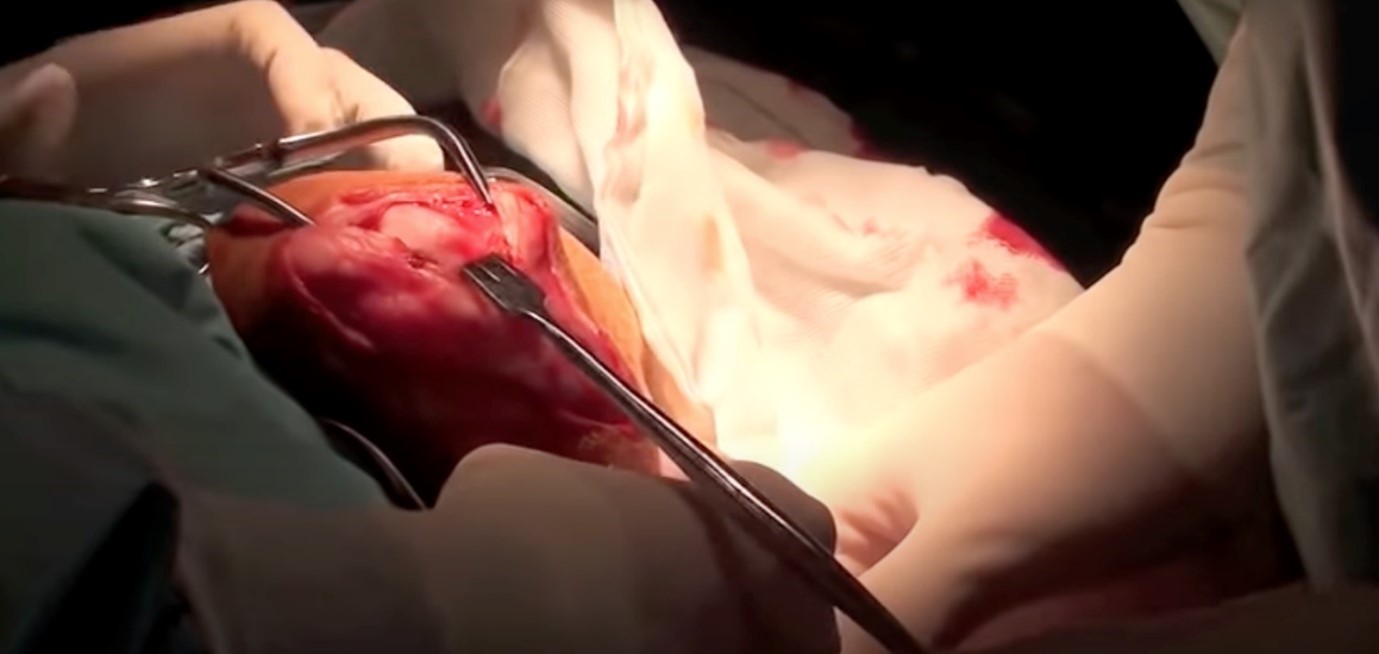
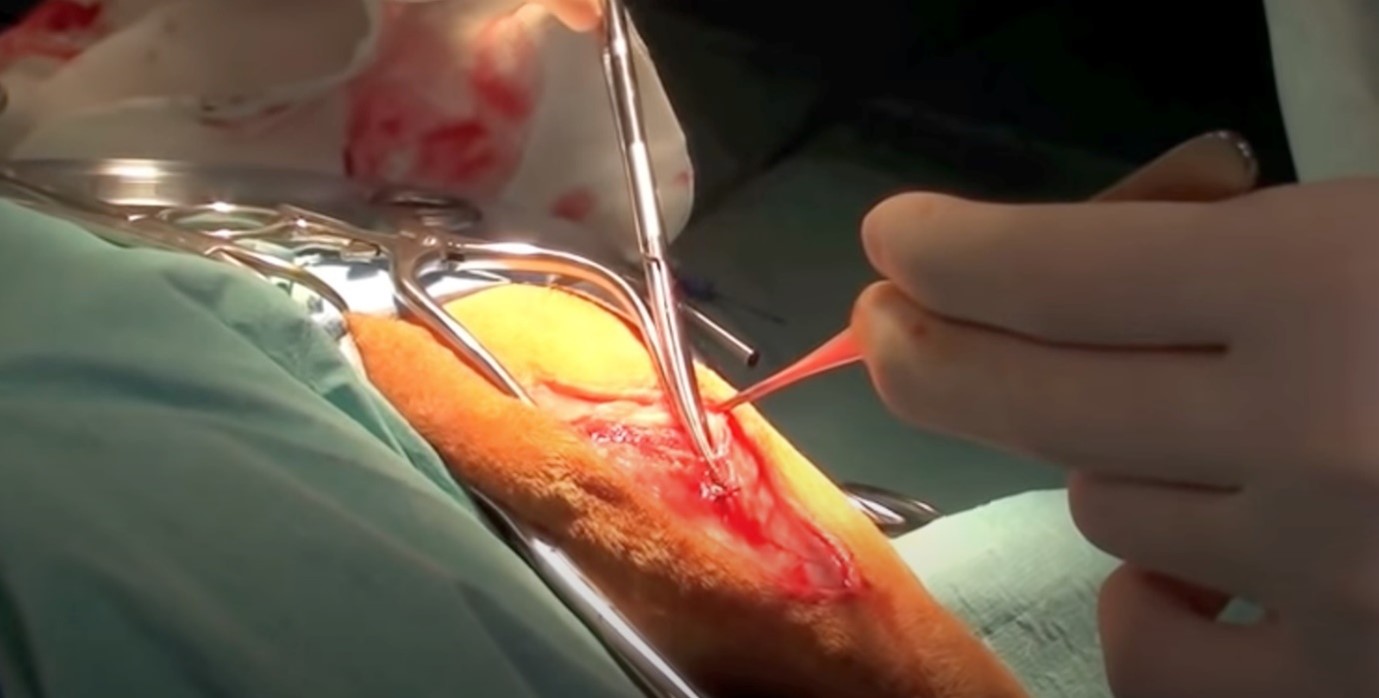
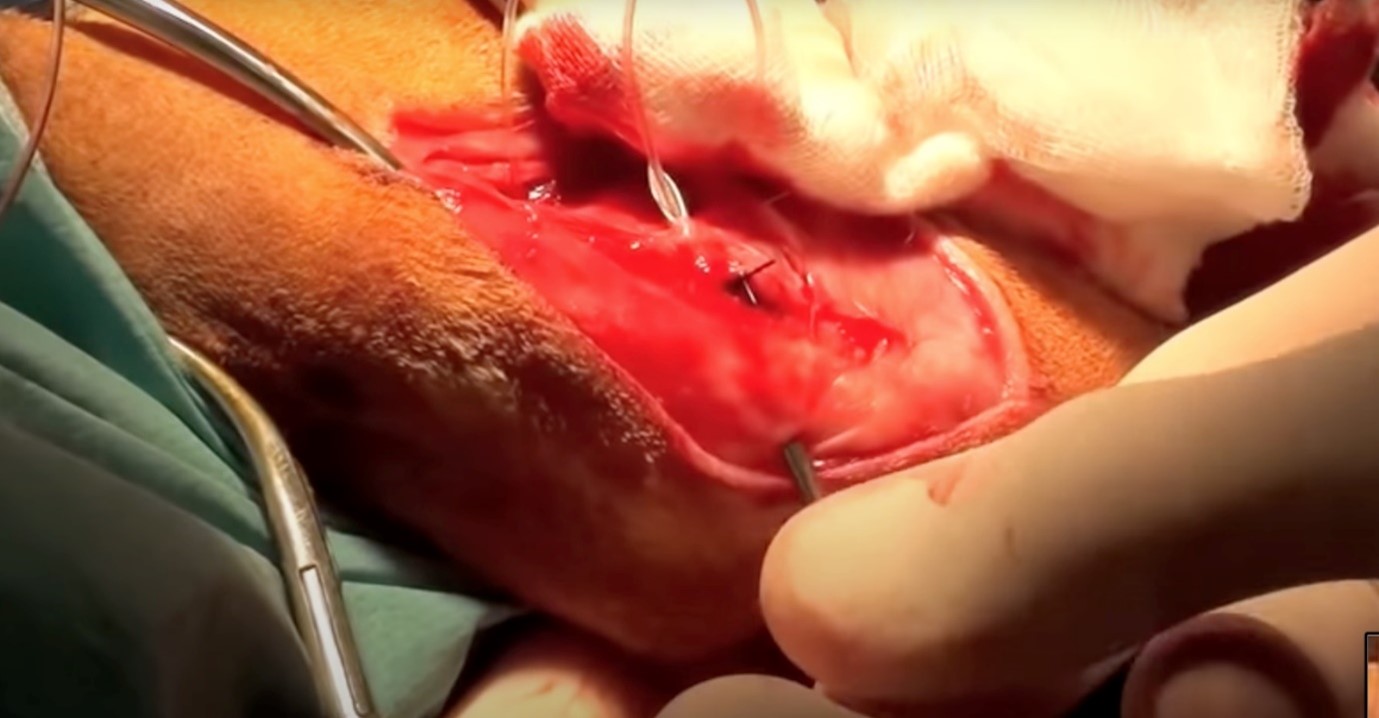
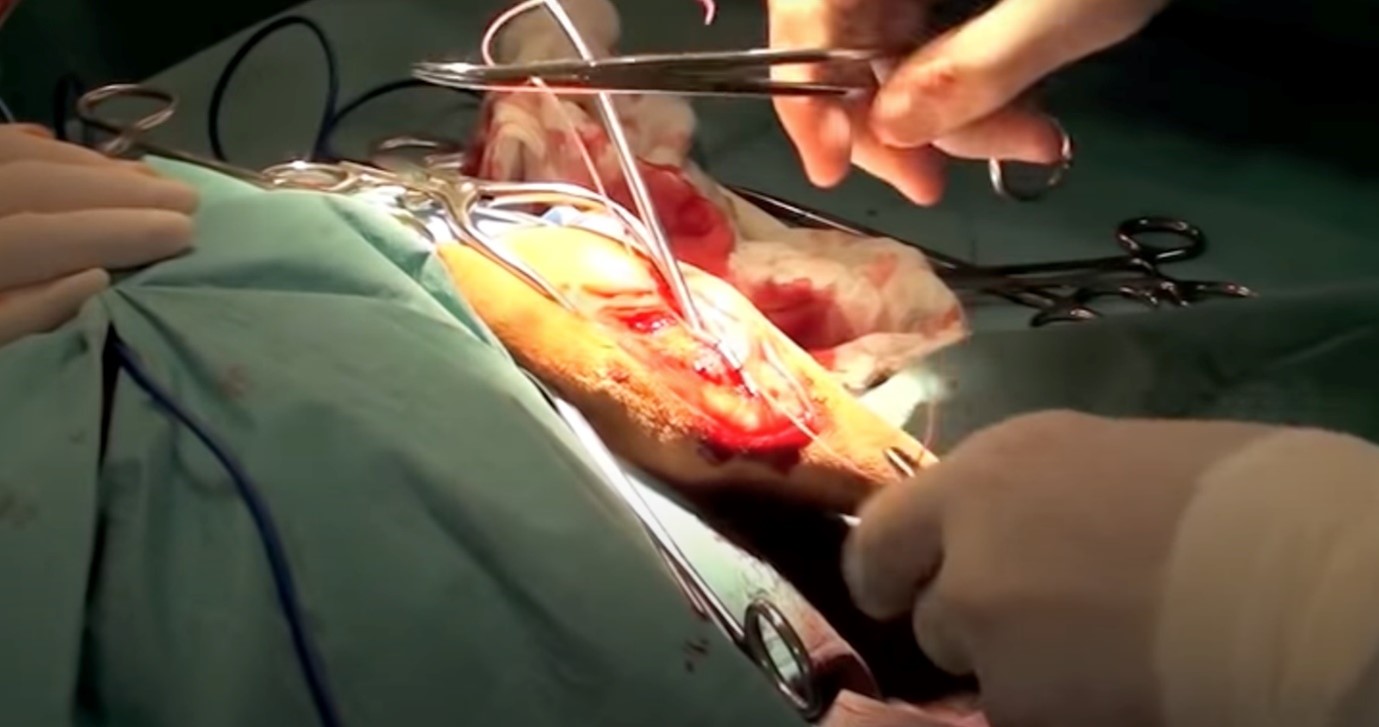
Extracapsular Repair For Dogs
By Dr Charles Kuntz DVM, MS, MACVSc, Diplomate ACVS, ACVS Founding Fellow of Surgical Oncology, Registered Specialist of Small Animal Surgery, Senior Staff Surgeon
How to perform extracapsular repair on a dog
You can read more of our specialist veterinary news and stories here.
For referring vets, please use our online referral form to submit a case enquiry.
Our Network
Animal Referral & Emergency network is the largest specialty and referral network in Australia, consisting of over 20 sites. With over 1,200 dedicated team members, including over 600 nurses and over 390 veterinarians (including specialists and registrars), we provide exceptional care for your pets. Count on us for expert medical attention and comprehensive veterinary services.